Leaderboard
-
TheOrcKing
Moderators18Points26,519Posts -
jaisonline
Moderators8Points10,854Posts -
$20 on joe vs dan
Members+6Points4,539Posts -
Pseudoty
Members+5Points7,497Posts





Popular Content
Showing content with the highest reputation on 03/31/2020 in all areas
-
6 points
-
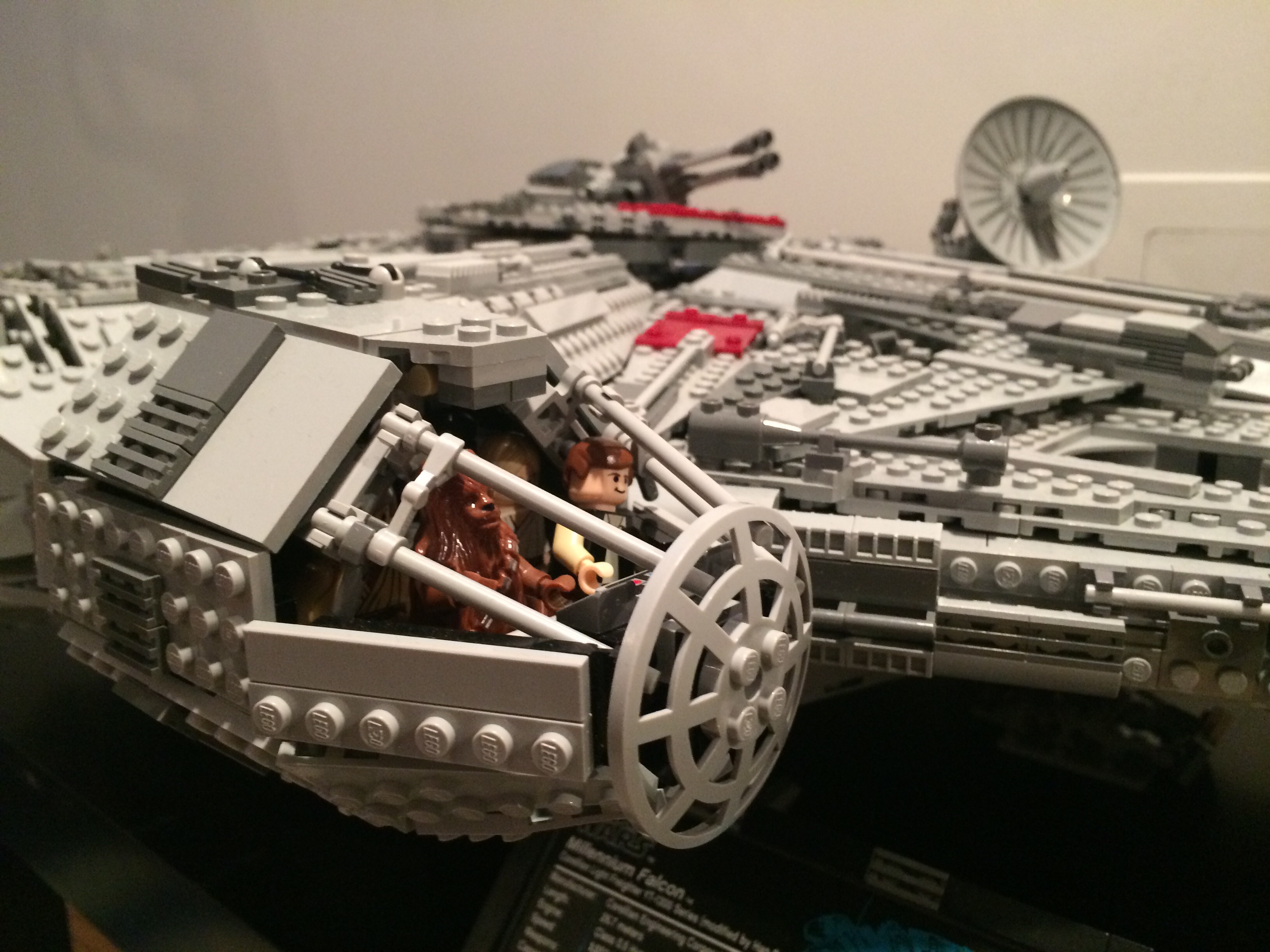
5 pointsWe finished the UCS Blockade Runner on Sunday. Man...what a beast of a set. Beautiful. Up next to build from the lot: UCS Death Star II, which was missing 4 pieces. @Huskers1236 I went with Vinyl aftermarket after seeing the shape the original stickers were in (as you can see in the pics) and reading online. They aren’t here yet, and it will be my first experience with aftermarket stickers.



 5 points
5 points -
4 pointsLet's put this to rest...face masks of almost any kind reduce virus spread. Whether it's a lot or a little, it does. It's a physical barrier. That being said, I realize why the government (Feds, CDC, WHO, Surgeon General, Etc...) would recommend against it...they are trying to stop hoarding and put the available masks in the hands of doctors and nurses. If they weren't effective, why are doctors and nurses wearing them? That is all...4 points
-
Someone asked me for a deal on the 10247 Ferris Wheel and 10257 Carousel together on a local auction site. I gave him a deal at $318US each, and now he wants to buy all the stock I have of those sets (total 6 more) at the same price. Average buy-in was $148. Sure, maybe I could sell them all between now and Christmas for up to ~$370, but selling the lot of 8 at once for $2544 with no fees is pretty worthwhile in my books The same guy also interested in buying my 4 Brick Banks and a bunch of other sets... Fingers crossed!4 points
-
3 pointsKinda like condoms when HIV began or seatbelts. During the Spanish Flu in 1918 it was mandatory to wear face masks in some cities in the USA. In 2 weeks it will be the norm but they can’t call them masks because that would be contrary to their message they will be called face covers or something like that and you will be required to wear one to go food shopping. Wearing a N95 mask at Walmart today does give you the feeling like wearing a Cowboys jersey to an Eagles game but I have seen the change. 2 weeks ago maybe 1 or 2 other people with masks last weekend about 30% of people wearing gloves and 10% wearing masks and I bet all the people wearing gloves would be wearing masks if they could get them.
 3 points
3 points -
My UPS guy said the volume is approaching Christmas levels.3 points
-
Post Offices and their employees need revenue also. Denying them business will not be good for anyone. I had a visit with our local Postmaster. He said with any downturn in revenue, it means higher future costs or layoffs.3 points
-
3 points
-
 3 pointsiahawks550 posted the IHME link yesterday. It's nice to see that at least the variance bars have tightened with the most recent update. I still think this study is **** ****, though, and I say that as a professional in the medical industry and a data scientist. They post their data, but they don't describe the statistical methods they use to arrive at their conclusions, there is no evidence of peer review (the "pics, or it didn't happen" test in my world), and as best as I can tell the information used by those models does not include intervention events. With a proper description, I should be able to recreate their results, but there is not enough model description for me to do so in practice. In my state (MA) their models is not tracking the reported stats, nor being adapted to current conditions (again, as best as I can tell, because the model is opaque). For good hard data, I've found this site to be valuable: https://covidtracking.com/. The numbers I'm watching are confirmed case counts, hospitalizations, and deaths. Hospitalization/dealts are running ~10%/~1% of confirmed cases. If capacity (beds, ventilators, etc) is reached, then the death rate will go up. If capacity can expand, the rate will likely stay static. If the therapy trials prove to be effective, it will drop. The big question, that no one knows the answer to yet, is what is the rate of asymptomatic cases which require neither testing or hospitialization? In short, I suggest one treat these models with skepticism. I think they are useful for predicting peak activity, but not total numbers. Don't despair or be led into fear by academic click-bait. p.s. ICU cases in MA are running 20-25% of total hospitalizations [cite: from my employer's daily update]3 points
3 pointsiahawks550 posted the IHME link yesterday. It's nice to see that at least the variance bars have tightened with the most recent update. I still think this study is **** ****, though, and I say that as a professional in the medical industry and a data scientist. They post their data, but they don't describe the statistical methods they use to arrive at their conclusions, there is no evidence of peer review (the "pics, or it didn't happen" test in my world), and as best as I can tell the information used by those models does not include intervention events. With a proper description, I should be able to recreate their results, but there is not enough model description for me to do so in practice. In my state (MA) their models is not tracking the reported stats, nor being adapted to current conditions (again, as best as I can tell, because the model is opaque). For good hard data, I've found this site to be valuable: https://covidtracking.com/. The numbers I'm watching are confirmed case counts, hospitalizations, and deaths. Hospitalization/dealts are running ~10%/~1% of confirmed cases. If capacity (beds, ventilators, etc) is reached, then the death rate will go up. If capacity can expand, the rate will likely stay static. If the therapy trials prove to be effective, it will drop. The big question, that no one knows the answer to yet, is what is the rate of asymptomatic cases which require neither testing or hospitialization? In short, I suggest one treat these models with skepticism. I think they are useful for predicting peak activity, but not total numbers. Don't despair or be led into fear by academic click-bait. p.s. ICU cases in MA are running 20-25% of total hospitalizations [cite: from my employer's daily update]3 points -
3 points
-
2 pointsIf everyone wheres one, no more stigma...which is the first hurdle that needs to be addressed. Tons of reasons why NOT to wear one, but if we're looking at the worse case scenario of someone who is sick WITH symptoms spewing contaminated droplets everywhere...there is a ton of data that says a mask will reduce that spread significantly...and if it takes everyone to wear a mask to "make" that sick person wear his...then during this time, shouldn't we do it?2 points
-
2 points
-
2 points
-
2 points
-
2 pointsThe USNS Comfort is a USNS ship, not a USS ship. It is operated almost strictly by civilian personnel and military and reserve medical personnel and the ship normally has a skeleton crew while in port. The rest of the crew are only called in once a emergency happens and the ship is ordered to respond. From what I read, the boat was in a maintenance period, which could have meant that engines were being worked on and repaired, or even replaced. Most supplies are removed from ships as well during maintenance availabilities, so they may have had to find more of those. I don't know if you have ever been around the lowest bidding companies that win the government contracts to repair our ships or not, but they are extremely slow and inefficient. Ships are often delayed coming out of overhaul periods by months or even a year. Plus, add in the fact that the reserve military medical professionals who sail on these ships aren't just sitting around twiddling their thumbs waiting for a emergency to happen. These are doctors and nurses from hospitals all over the country. And these hospitals are now a little less well staffed when USNS Comfort and Mercy are stood up.2 points
-
2 pointsI still don’t know how to time stamp YouTube videos but please go to 38:30 and watch for 1 minute And hear it from the horses mouth himself. Then we can finally put to rest the airborne transmission should we wear masks argument.2 points
-
2 pointsUsed Complete R2D2 $179 plus tax and $10 Shipped on Ebay I thought this one was never going to make it to my collection, but it's a great price; especially in this environment2 points
-
2 points2 years of Keto diet went down the drain thanks to the quarantine. At least that was my excuse for eating this huge bag of Lays2 points
-
2 pointsIt does to me too. I would have preferred a Creator model, but if my only option is Technic Mopar, then I'll take it, but I will be looking for a discount.2 points
-
2 pointsBroke out my 10226 Sopwith Camel and finally built it on Saturday. Got a bad lot of reddish brown as I broke 10 1x2 plates during the building. That and dark red seem to be the worst for brittleness. Plane is really cool and was a pretty fun build. Cool to see the mechanism come together at the end for the moving wings. I think the Maersk EEE is up next.2 points
-
2 pointsMy buddy held a Lego build a castle challenge over the weekend through our FB family. We were encouraged to use whatever Lego we had "around" the house. Those without kids like me were encouraged to join as well. With most of my loose Lego in storage I decided to bust open a water damaged 10237 ToO. I made sure to say it was a set and not custom. Took me about 15 hrs I'd say. I liked the build and it looks awesome. Now to break it down I guess.
 2 points
2 points -
2 pointsLittle bit of a flex here. Our new brand of Hand and Power tools, Blue Ridge, is now available at Target. There have been 20V tools and 40V OPE tools on Amazon for a little bit now, but this is our company's first venture into non-powered hand tools; of which I was integral to the 8-month compressed launch timeline. https://www.target.com/s?searchTerm=blue+ridge+tools In store, you might see some discounted Stanley, B&D and others tools since we have the entire 4 to 8ft section. Many are not shipping any longer but may still be available in store. These tools are good for entry-level homeowners and people who need quality tools for common household tasks. They are not Dewalt or Milwaukee quality, but are aimed to meet he needs of the common Target customer. Anyways, wanted to share as I am excited to see our team's hard work come to fruition.2 points
-
2 points
-
2 points
-
1 pointI wanted to create a new thread in order to give progress on my site updates. I want explain a bit on what happened and what I am doing. What happened with the site? Honestly nothing really exciting or dramatic, overall in the end, I did not want to support the host I was with for the past four years after not really offering too much help with managed servers. They would spend 30 seconds looking, say they can ping the server so its up and then just say, "hey not my problem". I was on aging hardware, paying the same amount of money, so I took the opportunity to move to a new host with better/faster hardware and a staff that does help to support you when run into an issue that you can't handle on your own. I have been doing this a long time and pretty good monitoring and handling 99% of what comes my way, but there are issues that you need the next level up to help figure out what to do. I wasn't getting anything like that, but paying for it. Not anymore. What my goal is... I know more than anyone that the site needed some TLC. It's been a while since I have done any drastic updates, the site looked tired and I know the site can be so much better than what it's current state was. LEGO investing has changed since Ed and I launched the site and it's time to remove the dead content and bring more of what people are looking for. Below is the short term list of items planned for updating. I have been working on the nightly, just like the early days and enjoying seeing parts of it coming to life. Fix the login. This has been messed up and quirky for a while. This has been resolved and working well. It's a simple thing overall, but nice that it actually works how it's supposed to Overall price guide site design update. The site was tired and disjointed. I hated it and pained me to look at it. Time to start over. Brickfolio update. All the Brickfolio data is safe. I have close to three million rows of data for Brickfolio entries. Time to bring this thing to 2020. I will probably create another thread at some point to solicit some feedback on some new requests for the brickfolio Fix the data syncing with Brickset. A lot of people used this feature, but it's time to make it work the way it should. Later I will work on the content portions. The news and blogs. I have some good ideas for this, but want to get the price guide and brickfolio to you sooner than later. What I am asking for if possible... If you can, please stop asking where the brickfolio is. Again, the data is safe and I am working as fast as I can to bring it all back to you. It won't be a few days, but more like a few weeks, but it will be worth it. I setup my dev environment to push releases quick and easy. I want to create a true changelog so that you can follow updates to see what was done/fixed/new/removed, you know like what real software companies do. I really do appreciate your patience with this. It wasn't planned, but if there was going to be a time to do it, it was going to be now.1 point
-
In Germany officials say that using selfmade masks and the non n95 ffp1-3 masks will mostly prevent, that if someone is infected he wont infect others. Its about passive protection. At this point there is no evidence for those masks to protect actively. But at the first day I heard officials about that topic I thought its about preventing that people start to hoard. But anyways...in Austria and one City in Germany people have to wear masks from now on in public places like Supermarkets...1 point
-
I decided this week to wear a mask for grocery shopping when I know I'm going to get in peoples bubble to some degree (as aisles are barely 6' wide). I noticed two weeks ago about 15% of people wearing masks at Meijer, then last week more like 50% of people, this week I went to Aldi instead and it's more like 20% of people there, but the demographic skews quite a bit poorer there. It's certainly more awkward to interact with people with a mask on, but you just follow Tyra Banks advice from America's Next Top Model and smile with your eyes: "Smeyesing"1 point
-
1 point(these kids are from around where I live - Loveland, OH. Kala Rose (the singer) is awesome)1 point
-
1 point1 point1 point1 pointyour source web site, propublica is definitely better than avg for facts. thanks for sharing the article. found this interesting. "This past September, with the design of the new Trilogy Evo Universal finally cleared by the Food and Drug Administration, HHS ordered 10,000 of the ventilators for the Strategic National Stockpile at a cost of $3,280 each. But as the pandemic continues to spread across the globe, there is still not a single Trilogy Evo Universal in the stockpile. Instead last summer, soon after the FDA’s approval, the Pennsylvania company that designed the device — a subsidiary of the Dutch appliance and technology giant Royal Philips N.V. — began selling two higher-priced commercial versions of the same ventilator around the world."1 point1 point1 pointI think we should just move everyone over 60 and anyone with a preexisting condition to Florida, move all others into the remaining states, continue business as usual in all states except Florida. </duck>1 pointJust spoke to the FedEx guy and he said it's getting close to Christmas for him.1 pointIn WA state. It's really job to job. Ive a couple roof repairs(deemed essential) to get on right away. Also most of my clients would prefer to wait on main projects in living spaces now that there stuck at home. Good people, Many will line up some "essential" little jobs if things get dire. I see a lot less deliveries than even a typical normal march 31 myself and in surrounding neighborhood.1 pointQUICK, everyone start talking politics and get this thread LOCKED.1 pointWHO recommendations have to take into consideration supply constraints on masks. why issue a recommendation that has zero chance of being implemented due to lack of supply and could also precipitate societal panic? CORONAVIRUS is transmitted via respiratory mechanism. infected cough out droplets which contaminate surfaces or are inhaled by the uninfected. masks offer a chance to block both of these mechanisms of disease transmission. in the countries that have this disease best under control, masks in public are a critical component of that strategy. masks are also part of very pragmatic Dr. Scott Gottlieb's roadmap to reopen america. protect yourself. don't listen what you are being told. do what makes sense. by preventing yourself from getting infected or further spreading disease, you won't place a burden on the already taxed health care system. wear a mask if you have one when you go out in public. fabricate a mask if you don't have one. even if no else is wearing a mask, do it. when you go out to a store, put on a hoody, wear the hoody over your head. when you get home from shopping, shed all the clothes and take a shower immediately. another nursing home 40 miles down the highway just had 15 people die from COVID. this is besides the 2 homes in the town next to mine which has one home up to 17 people infected. if you have a nursing home in your 30 mile radius that is infected, you better believe there are infected visiting the grocery, pharmacy, whatever store you are visiting.1 pointWell, that goes against what the WHO is advocating: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks BTW, I wear a mask when I go out into stores, even before my wife and daughter got sick. Daughter is in the last day of her 72hr-no-symptom-cool-off-period, wife not yet.1 pointlol - maybe this is why walmart is finally screening employees showing up to work by checking their temperature. wth - they weren't already doing this? further validating why you need to wear a mask when you go out in public. https://www.cnbc.com/2020/03/31/coronavirus-walmart-will-start-taking-all-employees-temperatures-before-shifts.html1 point1 pointFinally a data scientist that I could have a beer with. Where have you been all my life?1 pointI want to know why it took almost a month to mobilize the Navy Hospital Vessels. Seriously..THIS is a Homeland security issue...freakin China built a 10K bed hospital in 10 days with contamination zones. And US Navy can't mobilize a ship docked on the same Coastline in less than a month? At first I was thinking the delays was to make the ship contamination proof (which would still be too long , but reasonable); but now they are saying the Ship will only take on non-CV pts to help local hospital only focus on CV. It's like we can send a drone missile attack on the other side of the planet in less than 24 hours...yet a few miles along the Atlantic Seaboard...1 point
1 pointBack in January when I first heard about this, I made it a priority to stock up. The last time I walked into a Wal Mart or store of any kind, was about a month ago. Viruses have no boundaries, or expirations dates. There is no science that proves COVID-19 will go away when it gets warmer out. I’m a relatively healthy person, but I have asthma. I’m part of the 20%. Being able to breath is a luxury for me, and a luxury no one should ever take for granted. All it would take is me breathing in respiratory droplets of someone who has the virus, and there’s a good chance I’ll need one of those ventilators. I’m literally terrified to even go for a hike outside, because I’ve seen photos of what this virus does to a persons lungs. This is a terrible thing that is happening all over the world. No one wanted it, but it’s here. We’re all at war with an invisible enemy. Now that the enemy is here, we all need to step up, do are part, and unite as a whole world. The faster we do that, the faster we defeat it, and the faster we can all go back to our daily lives.1 point1 pointA couple of things I have wondered while watching each episode: 1). How many pieces are in these builds? 2). How long does it take to break these down and put all the pieces back and reorganized so that they are ready for the next challenge?1 point1 point1 pointI won a Battle of Hoth-100% Complete-with Box (75014) set on eBay yesterday evening for $33.59 / $44.06 total (including shipping/tax) that will fit in nicely with the Hoth battle scene I am making. MOC pictures to follow.1 point1 point




















.thumb.jpg.2388d65c77b4486ba81fd9fb9fdd1a00.jpg)







